
Reference
Shoulder anatomy
Medically reviewed by Dr Kalman Piper, FRACS (Orth). Last reviewed 15 July 2026.
A plain-English guide to how the shoulder is built and how it works. Covers the bones, joints, rotator cuff and other muscles, the labrum and joint capsule, and the underlying reason the shoulder is both the most mobile and the most prone-to-injury joint in the body.
Bones
Three bones meet at the shoulder
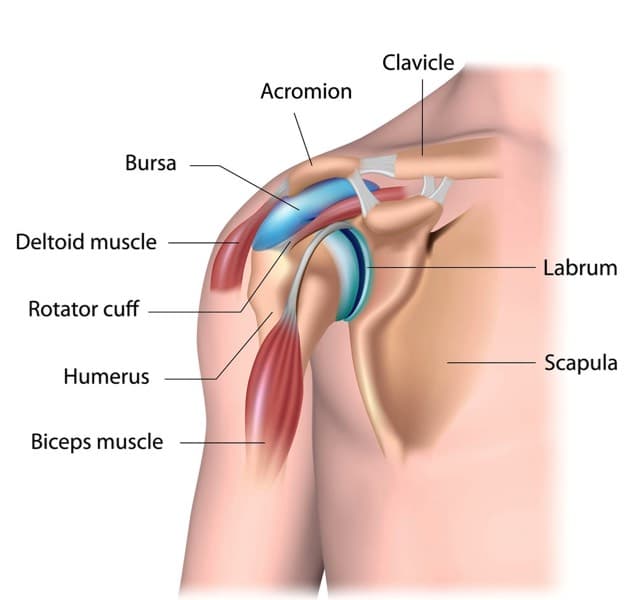
The shoulder is formed by three bones: the upper arm bone (humerus), the shoulder blade (scapula), and the collarbone (clavicle). Each contributes a specific part to the joints and provides anchor points for the muscles.
- Humerus. The long bone of the upper arm. Its rounded upper end forms the ball of the main shoulder joint. The humeral head is covered in cartilage and sits in the shallow socket of the scapula.
- Scapula. The flat, triangular shoulder blade on the back of the rib cage. It carries the socket of the shoulder joint (the glenoid) on its outer corner, the acromion above it, and the coracoid process at the front. The scapula does not have a rigid bony connection to the rib cage. It glides over the back of the chest as the arm moves.
- Clavicle. The collarbone. A long, slender bone running from the breastbone (sternum) at the front to the acromion at the top of the shoulder. It is the only bony connection between the shoulder and the rest of the skeleton.
Key landmark
What is the tip of the shoulder?
When people point to the top or tip of their shoulder, they are usually pointing at the acromion or the acromioclavicular joint (AC joint). Both sit at the highest point of the shoulder, just under the skin.
The acromion is a flat bony projection that comes off the back of the shoulder blade and arches over the top of the ball-and-socket joint. The outer end of the collarbone meets the front of the acromion. The small joint between them is the AC joint. It is held together by ligaments and allows a small amount of movement as the arm is raised.
Pain right at the tip of the shoulder, particularly with reaching across the body, lifting overhead, or lying on the shoulder, often comes from the AC joint. Pain just below the acromion is more often coming from the rotator cuff or the bursa underneath. Both are covered in more detail on the relevant condition pages below.
Joints
Four joints work together to move the arm
When people say "the shoulder joint" they usually mean the glenohumeral joint, the main ball-and-socket between the humerus and the scapula. But the full range of shoulder movement involves four joints working together in a coordinated rhythm.
- Glenohumeral joint. The main ball-and-socket joint. The ball is the head of the humerus; the socket is the glenoid on the outer corner of the scapula. The socket is very small and shallow compared to the ball, which is part of why the shoulder is so mobile but also vulnerable to dislocation.
- Acromioclavicular joint (AC joint). Where the outer end of the collarbone meets the acromion at the top of the shoulder. A small joint with a fibrocartilage disc inside. Often involved in falls onto the shoulder (AC joint separation) and a common site of arthritic pain at the top of the shoulder.
- Sternoclavicular joint (SC joint). Where the inner end of the collarbone meets the breastbone at the front of the chest. The only true bony connection between the shoulder and the rest of the skeleton.
- Scapulothoracic joint. Not a true joint in the anatomical sense (no joint capsule or cartilage), but the gliding interface between the shoulder blade and the back of the rib cage. The scapula rotates as the arm is raised, and this rotation accounts for around a third of total overhead reach.
Rotator cuff
The four muscles that power the shoulder
The rotator cuff is a group of four muscles that originate on the scapula and converge as tendons that wrap around the humeral head and attach to the upper end of the humerus. Their job is to centre the ball on the socket during movement, and to power most rotation of the shoulder.
- Supraspinatus. Sits on top of the scapula and passes under the acromion to attach to the top of the humerus. The most commonly torn of the four. Initiates lifting of the arm out to the side.
- Infraspinatus. Sits on the back of the scapula. External rotator of the shoulder (turns the hand outward when the elbow is at the side).
- Teres minor. Smaller muscle below the infraspinatus on the back of the scapula. Also contributes to external rotation.
- Subscapularis. The only rotator cuff muscle on the front of the scapula. Powers internal rotation (reaching the hand behind the back). The largest of the four.
The four cuff tendons blend together as they approach the humerus, forming a continuous cuff of tissue around the ball. When the cuff is torn, the tear is usually in this tendinous part rather than the muscle bellies.
For more on what happens when the rotator cuff tears, see the rotator cuff tear condition page.
Other muscles
Beyond the rotator cuff
The rotator cuff is the deep muscle layer. Several larger, more superficial muscles also act on the shoulder.
- Deltoid. The large muscle that forms the rounded contour of the shoulder. Its three heads (anterior, middle, posterior) lift the arm forward, out to the side, and backward respectively. The deltoid is the main lifter of the arm and becomes the primary mover after a reverse shoulder replacement.
- Biceps. Crosses both the shoulder and the elbow. The long head of the biceps tendon runs over the top of the humeral head and into the shoulder joint, where it anchors onto the upper rim of the labrum. Inflammation, partial tears, and detachment of this anchor (a SLAP tear) all cause pain at the front of the shoulder.
- Pectoralis major. The large chest muscle. Brings the arm across the body and internally rotates the shoulder.
- Latissimus dorsi. The broad muscle of the upper back. Brings the arm down and back, and internally rotates the shoulder.
- Trapezius, rhomboids, serratus anterior. Scapular stabilisers. They control the position and rotation of the shoulder blade on the back of the chest. Weak or poorly coordinated scapular stabilisers are a common contributor to shoulder impingement and other overuse problems.
Soft tissues
Labrum, capsule, ligaments, and bursa
Because the bony socket of the shoulder is so shallow, stability comes mainly from the soft tissues that surround the joint.
- Labrum. A rim of fibrocartilage around the edge of the glenoid socket. It deepens the socket, increases the contact area with the humeral head, and acts as the attachment point for several ligaments and the long head of the biceps. Tears of the labrum (Bankart tears at the front, SLAP tears at the top) are a common cause of shoulder instability and pain.
- Joint capsule. A tough sleeve of tissue that surrounds the glenohumeral joint and holds the synovial fluid that lubricates it. The capsule is loose enough to allow the shoulder its enormous range of motion, but tight enough to restrain the joint at the limits of movement. When the capsule becomes inflamed and contracts (as in frozen shoulder), the shoulder becomes painful and stiff.
- Glenohumeral ligaments. Thickenings within the joint capsule that provide static restraint at the limits of movement. The anterior band of the inferior glenohumeral ligament is the most important restraint against forward dislocation.
- Subacromial bursa. A thin, fluid-filled sac that sits between the rotator cuff and the underside of the acromion. It lets the cuff glide smoothly under the bone as the arm is raised. When inflamed (subacromial bursitis) it becomes a source of pain with overhead activity.
- Coracoacromial ligament. Runs from the coracoid process to the acromion, forming the front of the bony arch above the rotator cuff. Often trimmed or released during arthroscopic decompression surgery.
Nerves and blood supply
The brachial plexus runs through the shoulder
All the nerves to the arm pass through the shoulder region. They originate from the spinal cord in the neck, combine into the brachial plexus behind the collarbone, and then branch out to supply the muscles and skin of the arm and hand.
The two most important named nerves around the shoulder itself are the axillary nerve, which wraps around the back of the humerus and supplies the deltoid and a patch of skin over the outer shoulder, and the suprascapular nerve, which runs through a notch in the upper edge of the scapula and supplies the supraspinatus and infraspinatus. Both can be injured by dislocations, fractures, or compression.
The main artery to the arm is the axillary artery, which runs deep behind the collarbone and under the pectoralis major. It becomes the brachial artery below the shoulder.
How it works
Why the shoulder moves so far, and why it is vulnerable
The shoulder is the most mobile joint in the body. A normal shoulder can reach almost any point in space within an arm length. This mobility comes at the cost of bony stability: the socket is small and shallow, so the joint relies on soft tissues for stability rather than bony fit.
Lifting the arm overhead is not a single movement. It is a coordinated rhythm of the glenohumeral joint, the scapulothoracic gliding, the AC joint, and the SC joint, all moving together. As the arm goes up, the scapula rotates upwards on the rib cage, the clavicle rotates and elevates, and the humeral head spins on the glenoid. Disruption of any of these contributing movements can limit overhead reach.
Most shoulder problems are problems with one of these structures: the rotator cuff tearing, the labrum tearing, the joint capsule contracting, the subacromial space narrowing, the bony surfaces wearing, or the AC joint becoming arthritic. The condition pages linked below cover each in detail.
Conditions
Common conditions of the shoulder
Each of the structures described above can be the source of shoulder pain or dysfunction. The condition pages below cover the most common shoulder problems Dr Piper treats.
Rotator cuff tear
Detachment of one or more cuff tendons from the humerus. Pain and weakness.
Shoulder instability
Dislocations, subluxations, and labral tears (Bankart, SLAP).
Shoulder arthritis
Wear of the cartilage on the ball or socket. Includes cuff tear arthropathy.
Frozen shoulder
Inflammation and contracture of the joint capsule. Painful, stiff shoulder.
Shoulder impingement
Pinching of the rotator cuff and bursa under the acromion.
Calcific tendonitis
Calcium deposits within a rotator cuff tendon.
Clavicle fracture
A break in the collarbone, usually after a fall onto the shoulder.
Distal biceps rupture
A tear of the biceps tendon at the elbow.
Tennis elbow
Pain at the outer point of the elbow from extensor tendon overload.
FAQ
Frequently asked questions
- What is the tip of the shoulder called?
- The tip of the shoulder is the acromion. It is a bony projection from the back of the shoulder blade (scapula) that sits over the top of the shoulder joint. The acromion meets the outer end of the collarbone (clavicle) at the acromioclavicular joint (AC joint). When people point to the top of their shoulder, they are usually pointing at the acromion or the AC joint.
- What are the names of the shoulder muscles?
- The shoulder has four rotator cuff muscles (supraspinatus, infraspinatus, teres minor, and subscapularis), the deltoid (which forms the rounded contour of the shoulder), and the biceps and triceps which cross from the shoulder to the elbow. Larger muscles around the shoulder blade include the trapezius, rhomboids, serratus anterior, latissimus dorsi, and pectoralis major. The rotator cuff is the deep muscle group that centres the ball on the socket and powers most shoulder movement.
- What are the parts of the shoulder?
- The shoulder is made of three bones (the humerus, scapula, and clavicle), four joints (the glenohumeral joint, the acromioclavicular joint, the sternoclavicular joint, and the scapulothoracic joint), four rotator cuff tendons, the deltoid muscle, the labrum (a cartilage rim around the socket), the joint capsule and its ligaments, and the subacromial bursa. Together these structures give the shoulder more range of motion than any other joint in the body.
- Where is the shoulder joint?
- The main shoulder joint (the glenohumeral joint) sits between the ball at the top of the upper arm bone (humerus) and the shallow socket on the side of the shoulder blade (glenoid). It is below the acromion. A second joint, the acromioclavicular joint, sits at the very top of the shoulder where the collarbone meets the acromion.
- What is the front of the shoulder called?
- The front of the shoulder is formed by the coracoid process (a hook-shaped bony projection from the scapula that sits below the collarbone), the subscapularis tendon (the front-most rotator cuff tendon), and the anterior joint capsule and labrum. The biceps tendon runs through the front of the shoulder in a groove on the humerus. Pain at the front of the shoulder is often related to the biceps tendon, subscapularis, or anterior labrum.
- How does the shoulder work?
- The shoulder is a ball-and-socket joint with a very small, shallow socket relative to the size of the ball. This makes it the most mobile joint in the body, but also the least inherently stable. Stability comes mainly from the soft tissues around it: the labrum deepens the socket, the joint capsule and ligaments restrain movement at the limits of range, and the rotator cuff actively centres the ball on the socket during movement. The larger deltoid muscle is the main lifter of the arm.
Shoulder pain or stiffness?
Book a consultation with Dr Piper
Bring a GP referral and any imaging you have (x-rays, MRI, or ultrasound). Consultations at Lakeview Private Hospital, Norwest.